Process interview demo Video
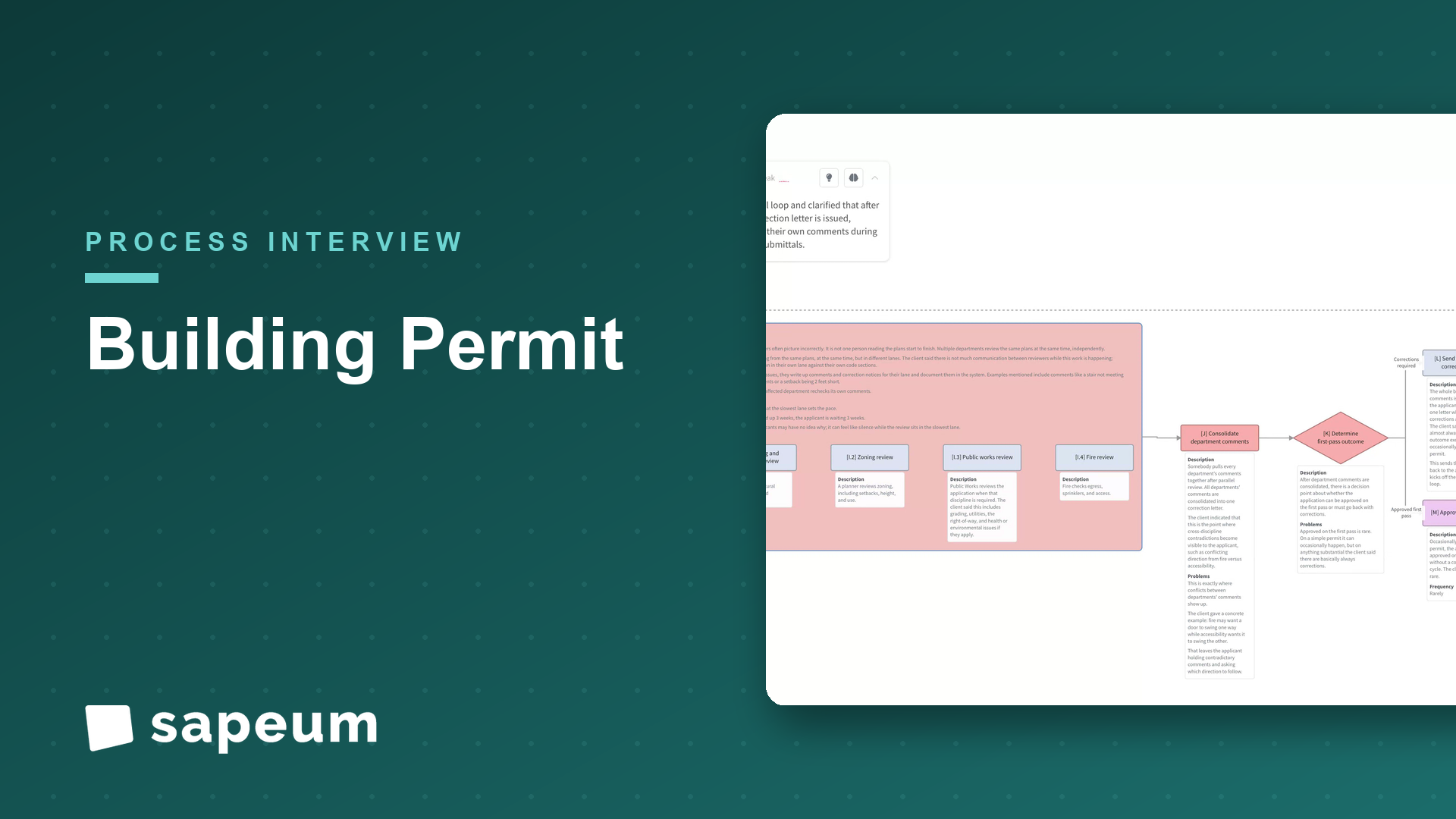
Building permits: submission to certificate of occupancy
A plans examiner maps multi-department review, resubmit loops, inspections, and final sign-off.
WatchA chief of staff at a mental-health telehealth company walks the half-year (H2) planning cycle end to end: from kickoff and the H1 retro through top-down guardrails, bottoms-up asks, clinician capacity by state, the trade-off room, and the tracking cadence that turns a plan into results.
Interviewer: Thanks for making time. I'd love to walk through how your H2 planning process actually works, start to finish, the way you'd explain it to a new exec joining mid-year. Wherever you want to start.
Chief of staff: Happy to. So just to frame it: we plan in half-years, H1 and H2, and the whole point of the cycle is to turn our strategy into a set of funded priorities and OKRs that every team is actually working against. I own the cadence of it. And it starts earlier than people expect. We're kicking off H2 planning well before H2 starts, late in H1, because it has to be done and approved before the new half begins.
Interviewer: What does kickoff actually look like?
Chief of staff: I set the calendar and the templates and socialize the timeline. It's timed around our fiscal calendar and the board meeting where the plan gets reviewed. One thing that can move it is if we're in the middle of a fundraise. That changes both the timing and honestly how aggressive we can be in the plan, because the amount of capital we expect to have shapes everything downstream.
Interviewer: Okay, so you've kicked it off. What's the first real input?
Chief of staff: The H1 retrospective. Before we plan forward we look back honestly at how H1 went against what we said we'd do. Member growth, clinician utilization; which is a huge metric for us; clinical outcomes, revenue, margin, our payer mix. We pull all that together so we're planning off reality, not vibes. And then alongside that, we refresh the external context.
Interviewer: Meaning the market?
Chief of staff: The market and the regulatory picture, which in our world is a lot. Telehealth reimbursement rules change, mental-health parity, state-by-state licensure for our clinicians, the controlled-substance tele-prescribing rules. The DEA stuff really matters for our psychiatry side. Plus competitors and what the payers are doing. All of that can open or close doors for the half, so we set it on the table before we commit to anything.
Interviewer: And then leadership sets the targets?
Chief of staff: Then the top-down guardrails, yeah. The CEO and CFO set the financial envelope for H2: the revenue target, the burn and runway we're managing to, and the headcount budget. That envelope is the constraint everything else has to fit inside. If runway's tight it's a more defensive plan; if we just raised, it's a growth plan. Then leadership agrees on the three to five strategic priorities for the half: things like expanding into new states, improving clinician utilization, rolling out measurement-based care, landing specific payer contracts.
Interviewer: So now the functions take over?
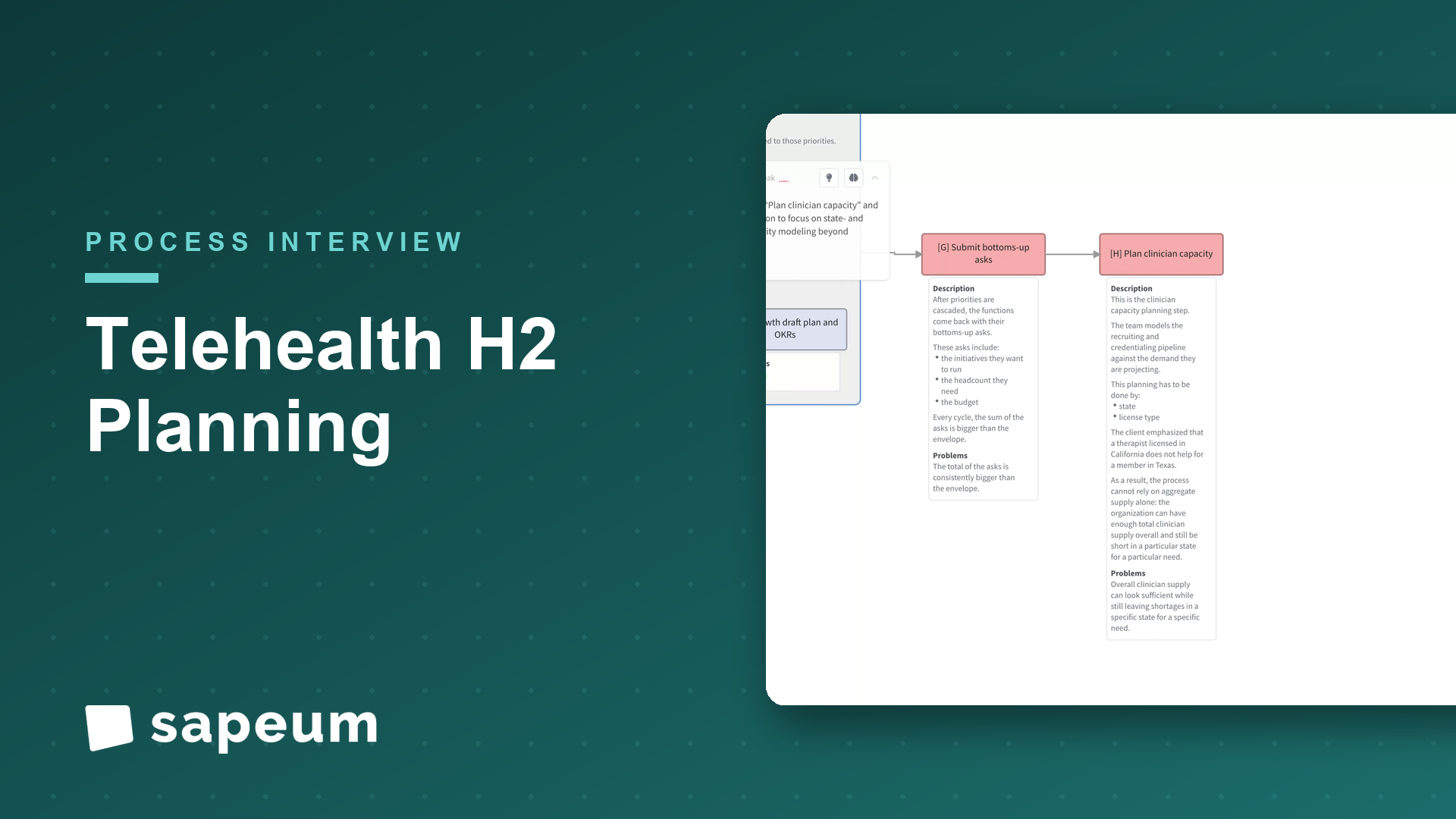
Chief of staff: Right, it cascades. Each function: clinical ops, product and engineering, growth, payer and partnerships, people; drafts their plan and their OKRs aligned to those priorities. And they come back with their bottoms-up asks: here are the initiatives we want to run, here's the headcount we need, here's the budget. And. Every cycle, without fail. The sum of the asks is bigger than the envelope. That gap is basically the whole game.
Interviewer: Before we get to closing that gap: you mentioned clinician utilization a couple times. Is there a planning step specific to that?
Chief of staff: There is, and it's the one that's most particular to a company like ours. We have to do clinician capacity planning: model our recruiting and credentialing pipeline against the demand we're projecting, and crucially, by state and by license type. Because a therapist licensed in California does me no good for a member in Texas. So we can have plenty of overall supply and still be short in a specific state for a specific need. When there's a mismatch, that gates growth: we either slow the marketing in that state or resequence the launch until the clinician supply is there. Getting that wrong means either members waiting weeks for care or clinicians sitting idle, and both are expensive.
Interviewer: That sounds like it touches a lot of other teams.
Chief of staff: It does, which is the next piece: mapping the cross-functional dependencies. Almost nothing we do lives in one team. Launching a new state needs licensing, a payer contract, clinician recruiting, and usually some product work, all lined up. So we lay out what depends on what, because an initiative that looks fundable in isolation might be blocked by something another team didn't prioritize.
Interviewer: Okay, now the hard part: closing the gap.
Chief of staff: Now the trade-offs. We get leadership in a room and reconcile the bottoms-up asks against the top-down envelope. Some things get fully funded, some get cut, some get resequenced to later in the half. That's the meeting that matters. It's where the plan is really made, because saying yes to everything isn't a plan. Then once we've made the calls, we lock the OKRs and targets: company level and function level, each with an owner and a metric. And FP&A finalizes the budget and the hiring plan tied to exactly what we funded.
Interviewer: And the board sees it.
Chief of staff: We take it to the board for review and approval. Sometimes they push back: they want more growth, or they're worried about burn. And we revise and re-cut. Once it's blessed, we communicate it. All-hands, managers cascade it to their teams, we publish the OKRs so everyone can see how their work ladders up. And then each team kicks off.
Interviewer: Is that where planning ends?
Chief of staff: That's where people think it ends, and that's the mistake. The last step is operationalizing it: setting the cadence to actually track against the plan. Monthly or biweekly reviews, dashboards, and a real mid-cycle re-forecast, because the world moves and a plan you set in June is partly wrong by August. And the results from this half become the retrospective input to the next cycle, so it's a loop.
Interviewer: So if you had to name the thing people get wrong about planning: what is it?
Chief of staff: Two things. One, people think planning is the goal-setting: writing the OKRs. But the OKR doc is the output; the actual work is the reconciliation, closing that gap between what every team wants and what finance will fund, and being honest in the trade-off room. Two, a plan without a tracking cadence is just a document. The teams that win are the ones that revisit it every couple weeks and adjust, not the ones with the prettiest planning deck in June. And for us specifically: the thing that quietly breaks a telehealth plan is capacity. If clinician supply and member demand drift apart by state, every other number in the plan goes sideways. So that's the part I watch hardest. And honestly, a lot of this still lives in spreadsheets and a dozen meetings, so keeping it all connected is its own challenge.
Interviewer: That's a great place to end it. Really helpful, thank you.
Chief of staff: My pleasure. It's a fun process to nerd out on, so anytime.
Keep exploring
A plans examiner maps multi-department review, resubmit loops, inspections, and final sign-off.
Watch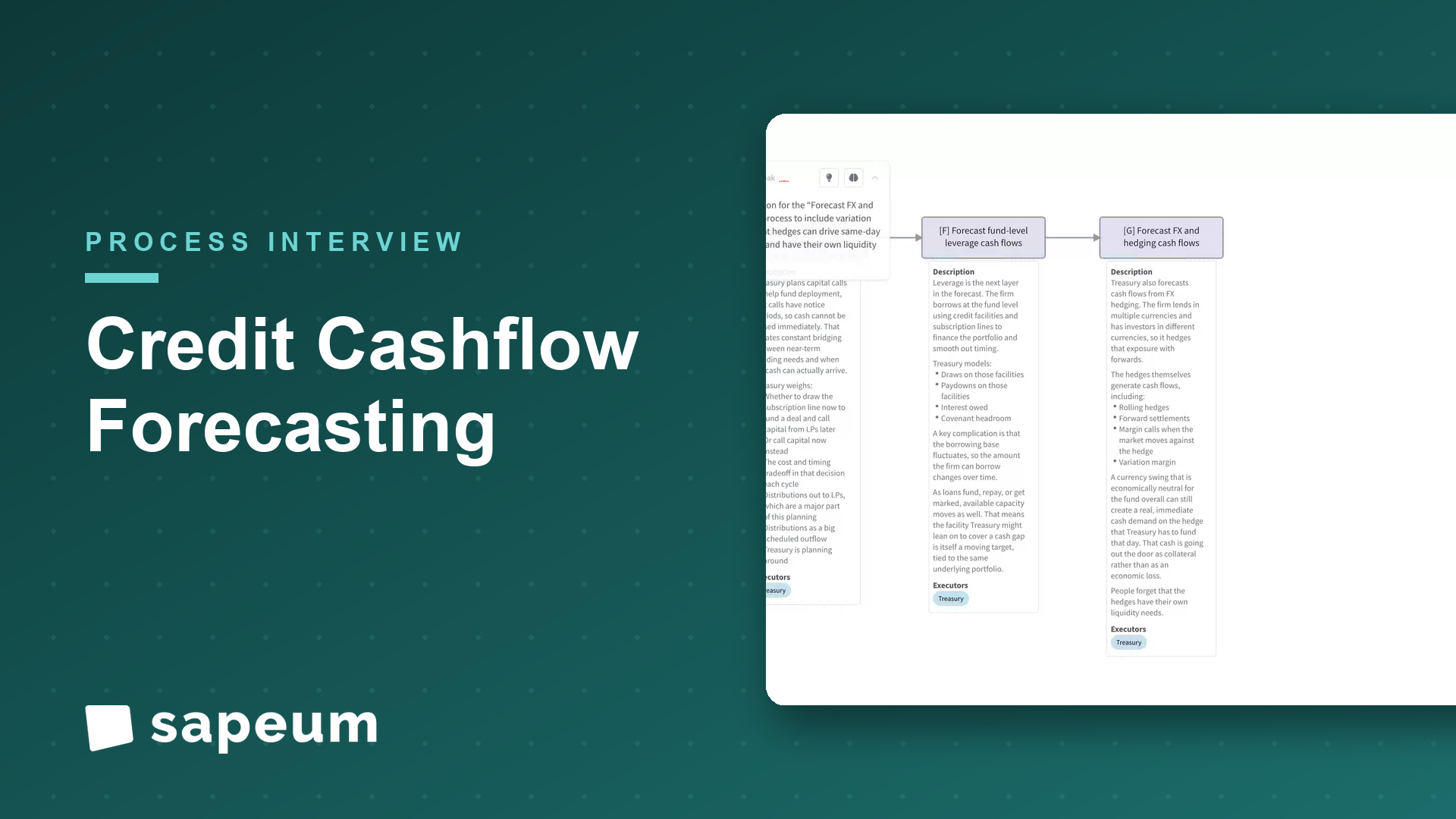
A treasury lead maps cash forecasting across funds and entities, and where it breaks down.
Watch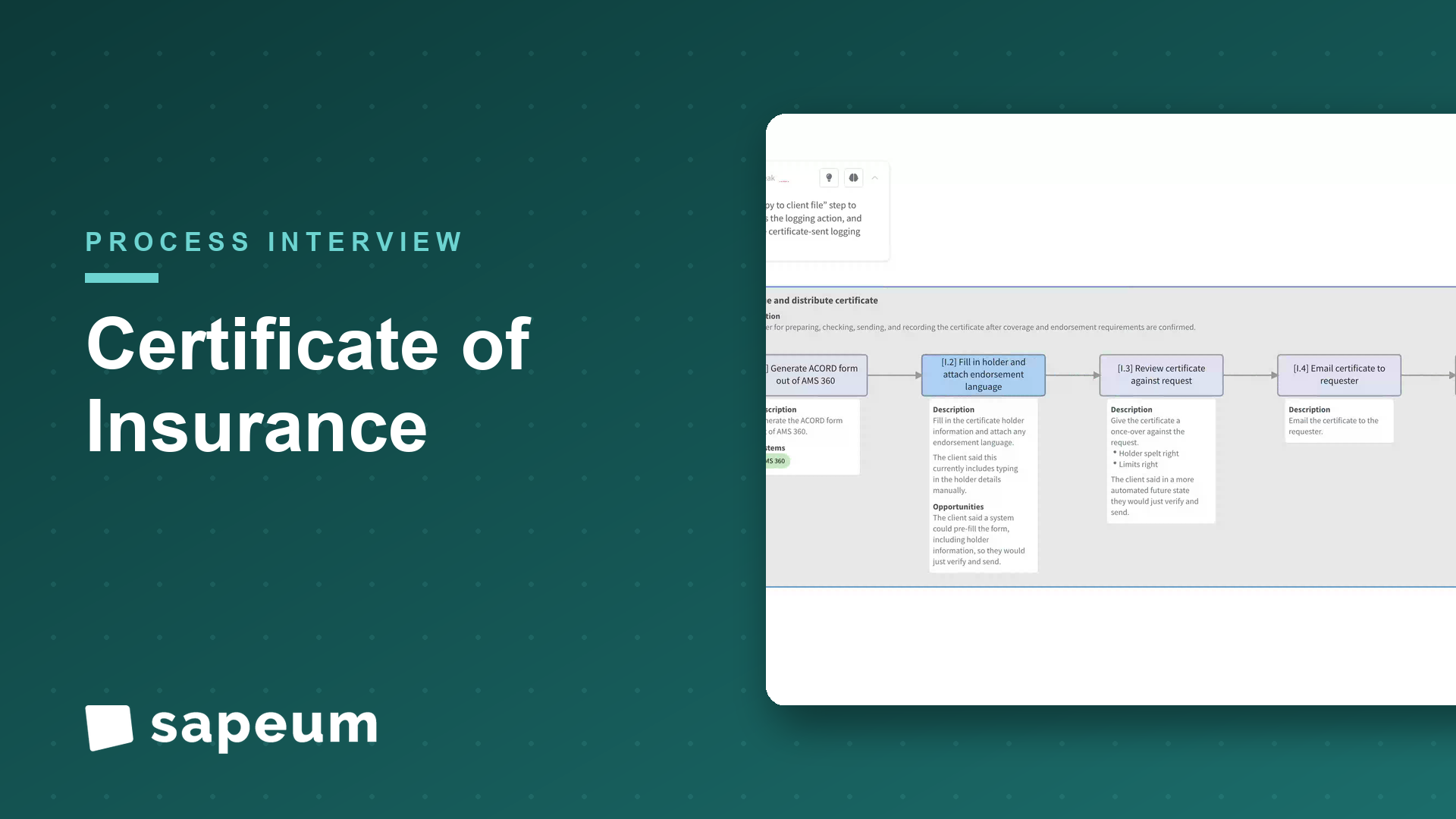
A brokerage account manager walks through COI issuance while the process maps itself; including the automation nobody had scoped.
WatchSapeum is designed with enterprise-grade security practices from the ground up: encryption at rest and in transit, role-based access controls, and auditable change history.
Everything you just saw runs on real workshops, not staged demos. Bring a process of yours and see for yourself.
Request a demo